
Open enrollment season is now upon us, and this year’s associated changes and confusion demonstrate Americans’ and lawmakers’ wide-ranging opinions on health care policy. Recently, several GOP leaders have tried to repeal Obama’s signature law, the Affordable Care Act, with the introduction of the American Health Care Act, the Better Care Reconciliation Act and the Graham-Cassidy bill. Contrast these to Bernie Sanders’s proposed “Medicare-for-All" bill, and we see a stark disparity in how different leaders are proffering to change health care. Amid legislative attempts supporting a free-market approach and some states’ efforts in expanding the government’s role in health care, larger conversations about system structure inevitably emerge. Often, universal health coverage, socialized medicine, and single-payer gain traction or opposition. However, these terms are frequently muddled together, producing unproductive dialogue within the health care debate. In clarifying these terms, we can better examine our own and other countries’ health care models to foster meaningful conversations about the ever changing and contentious US health care landscape.
Universal Health Coverage, Socialized Medicine, Single-payer
Contrary to common misconceptions, universal health coverage (UHC), socialized medicine and single-payer systems are not interchangeable terms. Rather, the World Health Organization broadly describes UHC as coverage for all members of a population for any kind of medical care (preventive, treatment, rehabilitation, palliative, etc.) that does not result in a significant financial burden to individuals. UHC is an umbrella term that socialized medicine and single-payer fall under; socialized medicine and single-payer systems may be implemented in an effort to achieve UHC. While socialized systems strictly integrate with the government, the government may or may not play a role in single-payer systems. A socialized system indicates that the government owns the buildings that provide care (e.g., hospitals, primary care clinics, urgent care facilities, etc.) as well as employs those who provide care (e.g., doctors, nurses, medical assistants, etc.). In a single-payer system, one entity pays for health care while hospitals, primary care clinics and other health care services are run by separate organizations, and doctors, nurses, and other health care providers are all employees of those organizations. Although it is true that the US uses a single-payer system for Medicare, and that payer is the government, single-payer does not dictate that the payer be the government. Theoretically, the payer could be any insurance company that obtained the entirety of the health insurance market. While these are general definitions, in reality, countries execute such systems in a variety of ways. The overall result is a unique system of and structure for care in each nation. Learn more about the variety of health care models below.
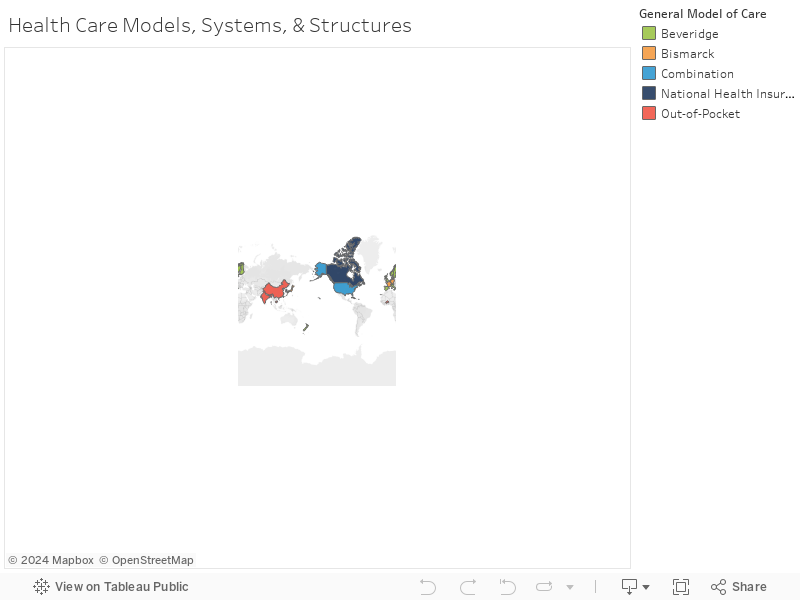
Hover over the colored countries for country name, the health care model used by that country, and in some cases, a more detailed description of that country’s system and structure. To move the map after zooming, select Shift+Click.
Four Models of Health Care
Four health care models used throughout the world are generally observed, providing insights into other countries’ systems of care. For each country that assumes one particular model, that country’s system also has its own structural nuances.
The Beveridge Model
The Beveridge model mostly aligns with socialized medicine but does incorporate some privately owned health care services. The model was name after William Beveridge, the economist and social reformer who helped establish Britain’s present-day health care system, the National Health Service. Hong Kong also uses the Beveridge model, unlike the rural areas of China.
The Bismarck Model
The Bismarck model relies on not-for-profit insurance plans to cover all people. In passing a bill that created “sickness funds” and the welfare state in Germany during his tenure, the model is named after Prussian Chancellor Otto Von Bismarck. In addition to Germany, parts of Latin America operate under the Bismarck model.
The National Health Insurance Model
In applying elements of the Bismarck and Beveridge model, The National Health Insurance model uses private sector providers, but the government acts as the sole payer of health services. While Canada is typically used as a primary example, Taiwan interprets the model in a slightly different way given its lack of a gatekeeper system.
Out-of-Pocket Model
The out-of-pocket model may be thought of as a lack of model; health care systems have not been established, and people must pay for their own care as needed. This often results in the rich receiving medical care and the poor going without. Along with Cambodia and Burkina Faso, rural areas in Africa and South America use the out-of-pocket model.
The United States: A Hodgepodge of Systems
The US employs aspects of all of these models into its system, but remains as the only industrialized nation that has not implemented some form of UHC:
- The Veterans Health Administration falls under the Beveridge model and is considered a socialized system.
- A plurality of US citizens utilize the Bismarck system by receiving coverage through their employer (note that in the US, insurance companies are for-profit).
- The government acts as the single-payer of health services for citizens aged 65 or older through the Medicare program.
- Some residents are uninsured and must pay for all health care costs out-of-pocket.
The US system borrows aspects of several different models that are not designed to work cohesively. While it has become clear that our system must change, the remaining question relates to how we will change. Perhaps we can look to other countries for guidance. For further reading on present day issues and recent legislation, please see the following:
About Jackie
Jackie Miller is a research analyst with the Institute for Health Policy Studies and Healthforce Center. Her projects focus on a range of research including community health workers, workforce policies and workforce supply and demand.