
By Sunita Mutha, MD, FACP and Jackie Miller
An imminent talent gap and provider burnout are threatening the viability and strength of California’s safety net, according to a newly released Healthforce Center at UCSF survey reflecting on-the-ground responses from senior leaders. One hundred and sixty-one safety net health care leaders across California responded to our survey, which aimed to unearth organizations’ biggest workforce challenges. Federally qualified health centers and community health centers are struggling to find, attract, and retain talent given financial strains and/or geographical locations. When leaders are able to onboard employees, they often face a consequent challenge; the safety net environment fatigues some providers, which risks pushing mission-driven providers away from the institutions that care for our most vulnerable populations. Problems with adequate staffing quickly impact other aspects of the organization, such as overall productivity, organizational finances and quality of patient care. Below is an overview of our findings, as well as solutions and recommendations to address these challenges.
The Talent Gap
When asked about their primary workforce challenges, safety net health care leaders most often reported their struggles to attract, find and retain top talent. Figure 1
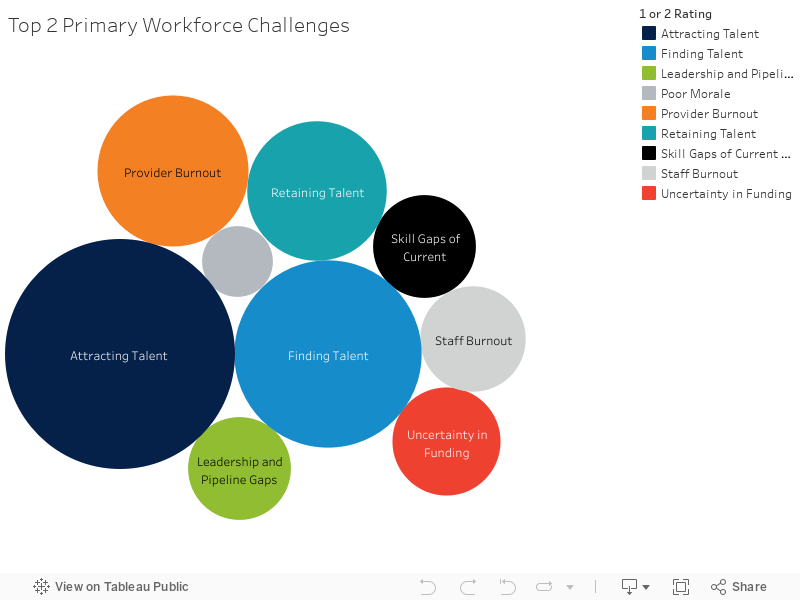
Among their most concerning primary workforce challenges, respondents rated the following:
- Sixty percent of respondents rated “attracting talent” as their first or second biggest workforce challenge
- Forty percent of respondents rated “finding talent” as their first or second biggest workforce challenge
- Twenty percent of respondents rated “retaining talent” as their first or second biggest workforce challenge
Leaders explained that they frequently observed challenges in these areas because they cannot offer competitive compensation packages and they struggle with issues related to their location within the state. One leader summed up these difficulties: “Top talent does not want to live in the Central Valley. If they do, they want to be paid above the 80th percentile.” Other respondents described their challenges as follows:
“If we can't attract talent, we can't provide quality services.” “Turnover is extremely expensive, undermines morale, stalls process improvement and negatively impacts patient care.” “[Turnover] contributes to staff/provider burnout and decreased morale. Constant training is very burdensome.”
Uncertainty in Funding Contributes to Staffing Challenges
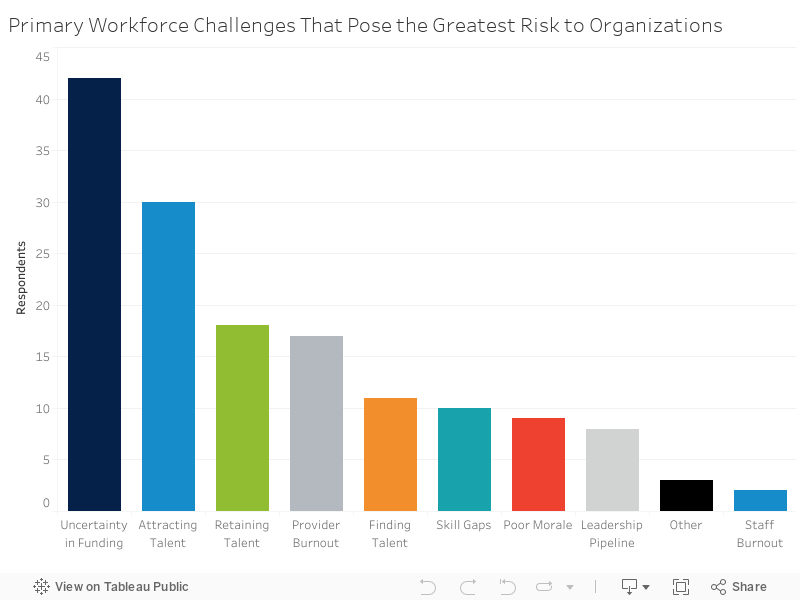
When asked about which challenges posed the greatest risk to their organization, the results indicate a slightly different story. While “attracting talent” (20 percent) and “retaining talent” (12 percent) are considered relatively large risks, as might be expected given that these were listed as some of the most important workforce challenges and biggest priorities, “uncertainty in funding” (28 percent) was considered the biggest risk compared to all other risk factors (Figures 2 and 4). One leader highlighted the inextricable link between adequate funding and obtaining a talented provider base:
“Uncertainty in funding can impact our ability to identify, attract and retain a highly qualified and mission driven workforce. As FQHCs, we just were approved for an additional two years of funding, but we immediately need to work towards more long-term funding. Furthermore, there are too many things that are still up in the air with Medicaid reimbursement. All of these together create a disincentive in working with FQHCs and could cause those already with us to look for jobs in the private sector.”
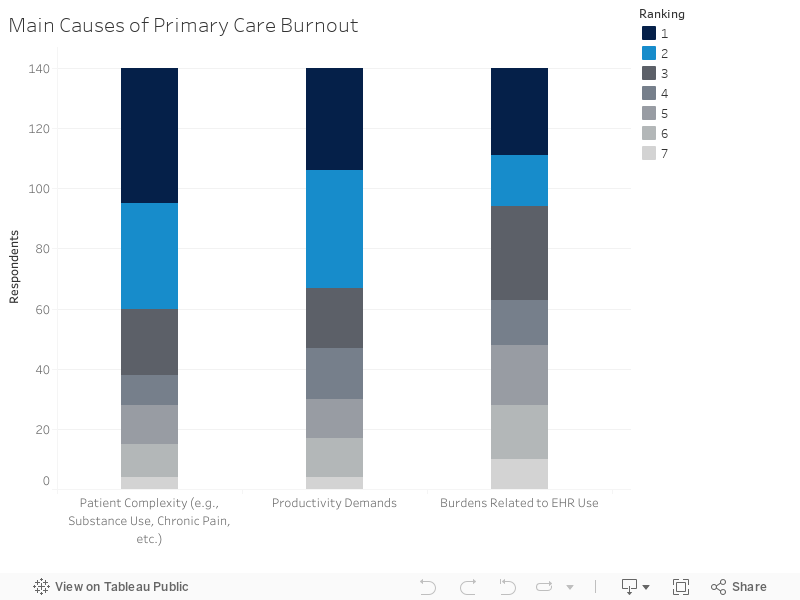
Burnout on the Rise
“Provider burnout” was also a major concern for surveyed health care leaders. Twenty-five percent of leaders listed it as their largest or second largest workforce challenge, and 47 percent of leaders listed it as a priority within their strategic plan. A couple of consistent trends tie together health leaders’ opinions on provider burnout compared to staff burnout. Double the amount of respondents rated “provider burnout” as their first or second primary workforce challenge compared to “staff burnout” (Figure 1), and respondents identified “provider burnout” as a larger priority that poses a significantly higher risk to organizations compared to “staff burnout” (Figures 3 and 4). Safety net leaders’ responses to questions about the causes of provider burnout offer more insights into how community health centers are grappling with this issue. Patient complexity and productivity demands stood out as the most frequently attributed causes of provider burnout, with 57 percent and 52 percent of health care leaders ranking them as the most or second most significant cause, respectively (Figure 5). Leaders explained that because “more and more [is] being asked of our providers,” this often creates “too little time with patients” and “difficult[ies] in getting specialty consults.” Furthermore, leaders expressed the interrelatedness of provider burnout and its effects on productivity, the bottom line, and, perhaps most importantly, patient care:
“We often lose providers and staff to other organizations, which impacts our quality of care and productivity.” “Without having qualified staff to see patients, we are unable to bill and meet financial obligations.” “[Provider burnout] leads to high turnover, poor care [and] unhappy patients.”
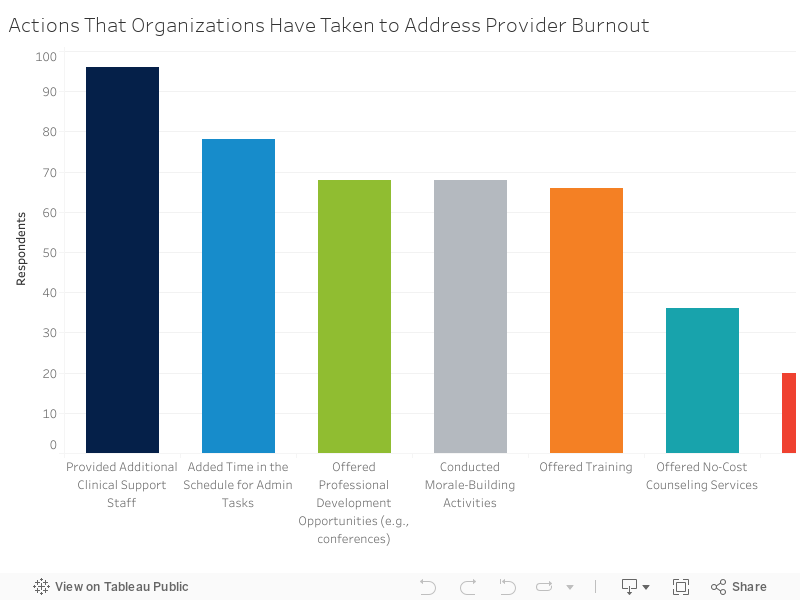
Leaders have adopted a variety of strategies to address burnout. Most safety net health leaders are providing additional clinical support staff (70 percent) and adding time in the schedule for admin tasks (60 percent). Additionally, another 50 percent of leaders are offering professional development opportunities and conducting morale-building activities, and 48 percent are offering training to combat provider burnout (Figure 5). Many organizations have added additional time in their schedules for admin tasks, professional development opportunities and training (Figure 6). While safety net leaders are taking action where they can, they are also thinking about the larger causes of and potential solutions to provider burnout. One leader expressed deep concerns about the health care system as a whole:
“I think providers are burned out because we have not fostered a system of high-functioning team care. We have been suspended in a state of implementation for too long, which is driving many good people to go to clinics where the team care model is better developed. In addition, we have allowed providers to dictate their schedules and productivity expectations, and have not incentivized quality of care. This has incentivized low-productivity and encouraged providers to stay, who otherwise may have left or adjusted their practice.”
Solutions and Recommendations
Although some of the questions raised can seem daunting, there are steps health leaders can take to address talent challenges and provider burnout:
6 Recommendations to Address the Talent Gap:
- Develop a “people infrastructure” as a top strategic priority. Investing in people should be a top focus for organizations. Leaders should involve their boards, stakeholders and staff members in a plan to nurture these most powerful assets.
- Get collaborative. Health leaders can provide training, support and incentives for team-based care. They should create a space where providers can discuss and share best practices for the most complex patients.
- Get flexible. Schedule predictable hours for those that need it and support a flexible schedule for those trying to balance caretaking and other responsibilities.
- Give the gift of time. Build time and resources (e.g., scribes) into providers’ schedules to allow them to meet productivity and documentation demands while still focusing on patient interactions, which are often a source of joy in a practice.
- Recognize and appreciate. One of the simplest ways to retain talent is to voice sincere appreciation for effort and to recognize a job well done, extra effort, or innovative problem-solving.
- Use technology. Invest in technologies, such as telehealth and electronic consultation and referral, that can maximize scarce provider resources, especially in rural areas.
6 Ways to Reduce Burnout in Safety Net Organizations
- Measure rates of burnout among providers. There are free or affordable resources leaders can leverage to assess levels of burnout within their organizations, such as the Maslach Burnout Inventory.
- Use Stanford University’s Professional Fulfillment Model as a framework. The model was developed to help health care leaders consider and strategize intervention possibilities. Drivers of professional fulfillment versus burnout fall into three major domains: efficiency of practice, a culture of wellness and personal resilience. A balanced approach that addresses each domain will drive long-term improvements in physician well-being and reduce burnout.
- Work with leaders involved in clinical operations to identify opportunities to include physician wellness in workflow decisions. Health care leaders should meet with frontline clinicians and ask:
- What elements in our workflow contribute most to stress or burnout?
- What are some things in our realm of influence that we could change to reduce burnout and increase professional fulfillment?
- Create a culture of compassion. This includes compassion for colleagues, patients and self. Encourage physicians to provide themselves with the same compassion they show their patients. Instead of judging themselves harshly when mistakes are made, a mindset of learning from mistakes will reduce stress and improve long-term effectiveness.
- Educate clinicians about sleep. Each single unit increase in sleep-related impairment (measured on a five-point Likert scale) was associated with 133 percent greater odds of self-reported burnout, according to Stanford Medicine’s 2016 Physician Wellness survey.
- Develop a stress management program. For acute moments of high stress, a critical event stress management program should be implemented at organizations. Schwartz Rounds, for example, offer providers and staff set monthly times to gather for presentations and dialogue during which they can openly and honestly discuss the social and emotional issues they face in caring for patients.
(source: California Improvement Network, CIN Connections, Spring Issue: Healing the Healer)
Referenced Figures:
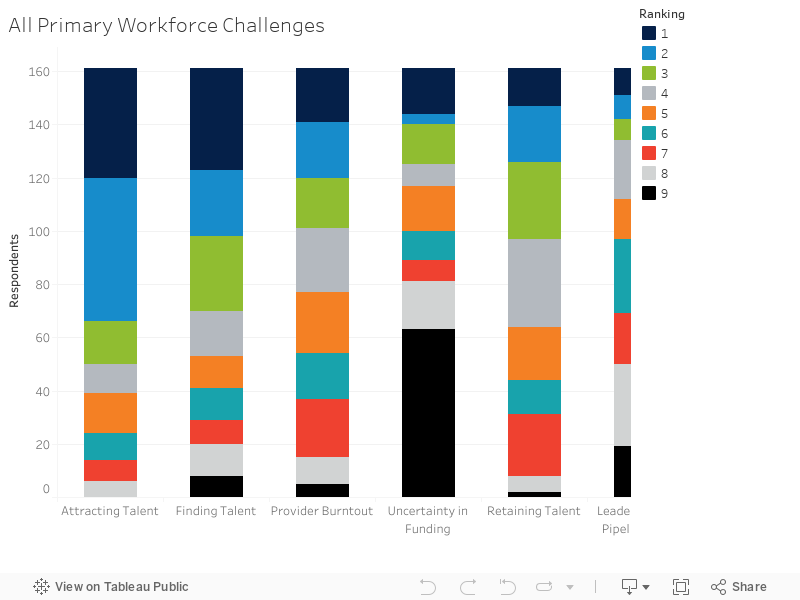
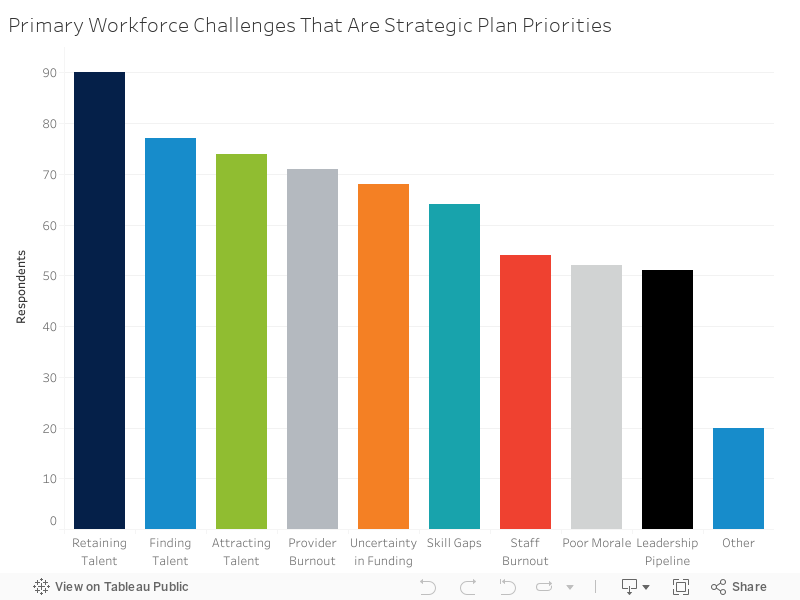
Figure 4
About California’s Health Care Safety Net
In California, community health centers serve more than four million people every year. They are the main source of health care for many low-income Californians, and they play a key role in providing care for underserved and vulnerable populations in particular.
Join Us
Healthforce Center at UCSF is the leading source for research insights into the evolving health care workforce and for pioneering training programs that empower leaders to navigate change. Sign up to get email updates on the latest health workforce trends and research, leadership development opportunities and stories of leaders who are driving change in the health care system.